Healthcare Outcomes Research Centre, RCSI University of Medicine and Health Sciences, Dublin, Ireland Received Date : 16 March 2023 , Accepted Date : 28 March 2023 , Published Date : 18 April 2023
Objectives: Little is known about the variation in health status by different population groups in Ireland. This study investigates the geographical variation in life expectancy (LE) and quality-adjusted LE (QALE) between Irish counties. Methods: Population numbers, mortality data and self-reported health status were obtained from the Irish Population Census and death registries. Census data from 2006, 2011 and 2016 were available by five-year age groups, sex and 31 counties. Mortality data were extracted for similar years. Standard life table methods were used to derive national and county-specific LE and QALE. Results: From 2006 to 2016, LE until age 85 increased in males (75.3 to 77.2 years) and females (75.3 to 77.2 years). Across counties, LE in 2016 ranged from 75.4 to 79.0 years for males and 78.0 to 80.7 for females. The proportion of the population self-reporting to be in very good or good health states was relatively unchanged between 2011 and 2016, but increased in those aged 50 to 84 years (p<0.05). Across counties, QALE in 2016 ranged from 71.5 to 75.8 years in males (average: 73.6 years) and from 73.4 to 76.1 years in females (average: 75.0 years). Sex differences decreased in LE and QALE from 2011 to 2016. Conclusion: Within a decade, LE, the health status of 50 to 84-year-olds, and QALE improved with substantial variation across counties. While sex differences decreased, county differences in QALE remained. Policymakers need to be aware of this de facto increase in health inequality.
Keywords:
Life expectancy , Quality-adjusted life expectancy , Geographic variation , Health inequalities , Self-reported health status , Census of Population.
Introduction
Population studies have identified regional variations in mortality and life expectancy (LE) between and within European countries [1-3] and
within countries outside of Europe [4-7]. Different time trends have been observed in geographic inequalities over the past 40 years. While studies have reported widening geographic differences in LE in Seoul [5], Columbia [6] and the US [8,9], geographic differences remained relatively stable across English regions and decreased in Norway [2,10].
Improvements in health status have led Ireland to become one of the top European countries with high levels of good or very good self-perceived health and a high LE [11,12]. For example, from 1984 to 2005, infant mortality decreased from almost ten to less than four per 1,000 live births [13]. Along with better access and availability to healthcare, different contextual factors have affected the health of the Irish population. For example, coal bans led to a general reduction in Irish respiratory mortality after 1998 while domestic accidents and self-harm increased morbidity during the 2008-economic recession [14,15].
Despite overall improvements in population health, a number of studies have identified geographic health inequalities in Ireland. In 2015, Masterson et al. found higher hospital mortality for patients living in rural compared to those living in urban areas [16]. Additionally, their study showed that statutory Emergency Medical Services responded to cardiac arrest by resuscitation slower and less often in rural regions [16]. Data from the National Cancer Registry indicate that many types of cancer were more prevalent in urban regions from 1995 to 2007 [17]. Using population-representative data, O’Farrell et al. identified geographic differences in suicide and self-harm in Ireland that indicate variation in health due to socioeconomic factors. In their study, the deprivation of some regions and, less so, social fragmentation and rurality were associated with observed geographic differences [18].
Findings by Corcoran and Arensman using data on self-harm from A&E registries in 38 Irish hospitals added further support to this finding [19]. Other studies found a higher demand for
acute hospital services in Ireland Northwest, West, and Midwest regions, driven by geographic differences in age and health status [20], and elevated use of free prescription medicines in the Midlands region of Ireland [21].
Developments in geographic inequalities of Irish health status have been investigated to a lesser extent. Studies have found that socioeconomic inequalities in health remained or increased from the 1980s to 2008 [22-24], while other studies suggest a reduction of inequalities in health and healthcare access. For example, regional differences and access to cardiac rehabilitation services improved from 1998 to 2003 [25,26].
Using data from the national Census of Population 2006, the Central Statistics Office (CSO) published a report indicating that Irish mortality and LE were unequally distributed across different geographic areas. This analysis was based on a deprivation index of small area population statistics and found that mortality was higher in urban than rural areas. Furthermore, LE increased with educational status and occupational class of Irish residents [27]. While data from 2016 confirmed that small area differences in mortality were associated with deprivation, educational status and occupation, lower mortality rates were observed for Dublin and Galway city and suburbs than observed in other areas the country [28]. Further and updated analysis of national and regional developments in LE is warranted. Additionally, investigations of LE adjusted for quality of life, and inequalities in quality-adjusted LE (QALE), are missing in Ireland.
The aim of this study was to investigate the development and geographic variation in LE and QALE in 31 Irish counties using population-level census data from 2006, 2011 and 2016.
Materials and methods
Study design
This study used the entire Irish population represented in the quinquennial censuses as national cohorts in standard life table models to estimate LE and QALE for the whole population and for populations in Ireland
31 geographic districts.
Setting
The Republic of Ireland has 4.8 million inhabitants (Central Statistics Office, 2016). The Central Statistics Office reports census data in 31 districts, namely different parts of Dublin (the capital, located in Ireland
Mid-East), three large city centres (Cork, Galway and Limerick) and counties centred around other cities and towns with population sizes ranging from 32,000 to 555,000 residents. This geographical division dates back to the Norman invasion of Ireland and was used to control taxes during the English occupancy and is currently used to organise the legal court system. Currently, these 31 districts demarcate areas of local government, but do not always follow the administrative boundaries of the health and social services.
Data sources
In this study, we used three waves of the Census of Population, collected in 2006, 2011 and 2016, and mortality data from the Irish death registry for the years of 2007 to 2016.
The Irish Census of Population is carried out every five years and participation is mandatory with high participation rates. Accumulated data on electoral district level are available from the Central Statistics Office
webpage. The full dataset includes detailed population counts and responses to the census survey organized in 15 themes, by sex and age, and for each electoral
district, as well as grouped for 31 counties, and for rural (i.e. population <1,500) vs urban areas. For the purpose of this study, we extracted population counts by electoral districts from the 2006, 2011 and 2016 Census. The 2011 and 2016 Census asked respondents to describe their current health state as ‘very good’, ‘good’, ‘fair’, ‘bad’, or ‘very bad’.
From the Central Statistics Office, we also downloaded a dataset of annual mortality that has been compiled based on local authorities’ reporting of deaths, by geographic area, sex and age. To match the Census data, we used mortality data from 2007, 2011 and 2016. Mortality data were not available for 2006; however, 2007 mortality data were assumed to be similar to the 2006 number of deaths.
Through careful mapping of the electoral districts in census data and the geographical areas used in the mortality data, we were able to compile accumulated data for each of the 31 counties on population size, self-reported health status, and number of annual deaths (all by sex and five-year age groups). We validated this mapped dataset against available national data.
Despite differences in administration of the census and death registry, the data material is considered to provide an accurate description of the population in Ireland [29,30].
Variables
For each geographical district, by sex and five-year age groups, we obtained the number of residents in 2006, 2011 and 2016, number of deaths in 2007, 2011 and 2016, and self-reported health status in 2011 and 2016.
Analysis
Initially, we conducted national descriptive statistical analysis (frequencies and proportions) for each year. Missing value analysis was performed for self-reported health. All other variables had no missing values reported and were assumed to be complete.
Using the above data sources, we used life table methods to calculate LE at birth in 2006, 2011 and 2016, and to calculate QALE at birth in 2011 and 2016. Sex-specific LE and QALE were calculated on state level, as well as separately for the 31 geographic districts. The calculations were truncated at 85 years of age due to the structure of available data. International sex-specific data on health status and EQ-5D health utilities were used as weights for the QALE calculation [31].
Changes over time were assessed using McNemar
test, and p<0.05 was deemed to indicate a statistically significant change.
Statistical variation like standard deviation and confidence intervals of LE and QALE are not reported because the dataset is comprised of complete national data. Statistical analysis was performed using Stata 17.
Results
Descriptive statistics
In 2006, 2.1 million males (50.0%) and 2.1 million females (50.0%) lived in Ireland. The population of males and females increased to 2.3 million (49.5%) and 2.3 million (50.5%) in 2011 and to 2.4 million (49.4%) and 2.4 million (50.6%) in 2016. While the share of children and adolescents (≤19 years) remained stable (27.2% in 2006, 27.5% in 2011 and 2016), the proportion of young adults aged 20 to 34 years decreased from 25.1% in 2006 to 19.6% in 2016 (a 22% decrease) and the proportion of those aged 65 years and older rose by 22%, from 11.0% to 13.4%.
Over the ten-year period, increasingly more people lived in urban areas (60.7% in 2006 vs. 62.7% in 2016), with fewer people particularly in the Mid-West and an increasing proportion living in the Mid-East of Ireland. In 2011, 60.3% of the population indicated to be in very good health (59.4% in 2016), 28.0% were in good health (27.6% in 2016), 8.0% were in fair health (equal in 2016), 1.2% were in bad health (1.3% in 2016) and 0.3% indicated that their health status was very bad (0.2% in 2016). Across the study period, just over 28,000 annual deaths were registered in Ireland. Appendices 1 and 2 show detailed population characteristics in 2006, 2011 and 2016, and changes in sex- and age-specific mortality over time.
Health status differences across sexes and age groups
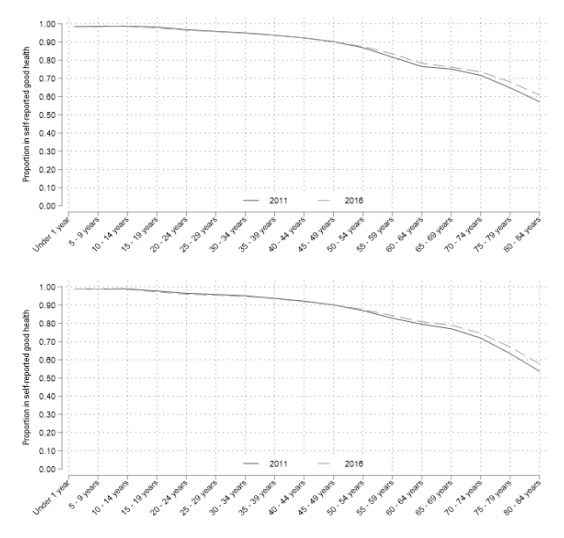
Most males (90.3%) and females (89.8%) reported to be in very good or good health in 2016 (Appendix 3). Self-reported health was highest in childhood and adolescence (≥97%) and decreased thereafter with steeper decreases seen from the age of 50 years. The lowest proportion (≤68%) and fastest decline in very good or good health was seen in the ages of 75 years and older. Three in four of those aged 55 to 84 years (range males: 57.8-84.4%; range females 60.8-83.5%) reported to be in very good or good health in 2016.
On population level, the proportion in very good or good health was relatively unchanged from 2011 to 2016, showing a small statistically significant (p<0.001) decline for males (-0.3%) and females (-0.1%). Specifically, significant declines of between 0.1% and 0.6% in this proportion were seen in both sexes and all age groups from 10 to 34 years (p<0.05), while no significant changes were seen in children below the age of 10 years and adults aged 35-49 years.
Simultaneously, significant increases of between 0.6% and 4.1% in the proportion of very good or good self-reported health were seen in all sexes and age groups from 50 years of age and older. Sex- and age-group-specific health status is displayed in detail in Appendices 3 and 4.
In 2016, LE until 85 years of age was 77.2 years for males and 79.8 years for females, reflecting an increase in both sexes since 2006. As male LE
increased more, the observed sex difference decreased from 3.4 years in 2006 to 2.9 years in 2011 and 2.5 years in 2016 (Table 1).
Based on the above numbers, QALE until 85 years of age increased from 72.6 in 2011 to 73.6 in 2016 among males and from 74.5 to 75.0 in females. Accordingly, sex differences decreased from 1.9 years in 2011 to 1.4 in 2016.
2006
2011
2016
Change
2006-2016
Change
2011-2016*
Life expectancy
Men
75.3
76.3
77.2
1.9
0.9
Women
78.7
79.2
79.8
1.1
0.6
Difference
3.4
2.9
2.5
-0.8
-0.4
Quality-adjusted life expectancy
Men
N/A
72.6
73.5
0.9
Women
N/A
74.4
75
0.6
Difference
N/A
1.8
1.5
-0.3
for quality-adjusted life expectancy, 2011 was the earliest year in which data were available. Table 1 : Changes in life expectancy and quality-adjusted life expectancy at birth until 85 years of age from 2006 to 2016.
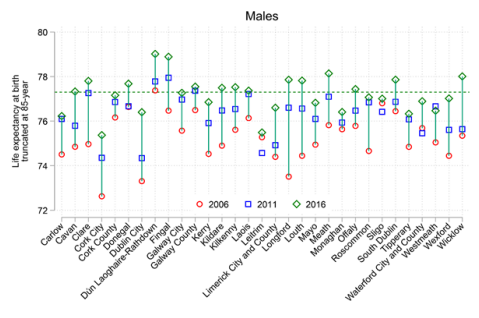
Across the counties, LE in 2016 ranged from 75.4 to 79.0 years in males and from 78.0 to 80.7 in females. More geographic variation was seen in males in 2006, decreasing from a range of 4.8 years in 2006 to 3.6 years in 2016. In females, the geographic variation was lower and changed only slightly, from 2.9 to 2.7 years between 2006 and 2016.
As depicted in Figures 1 and 2, LE increased between 2006 and 2016 in almost every geographic district; however, in some districts it increased more than in others, ranging from 0.2 to 4.3 years in males and -0.5 to 3.2 years in females. Decreases in LE were seen in females in Carlow and Leitrim.
Figure 1 : Geographic variation and changes over time in life expectancy at birth until 85 years of age across 31 districts in Ireland, males.
Figure 2 : Geographic variation and changes over time in life expectancy at birth until 85 years of age across 31 districts in Ireland, females.
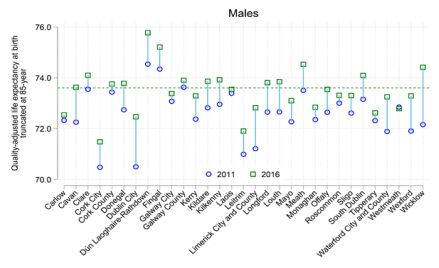
When adjusting LE for health status, a similar pattern was seen (Figures 3 and 4). Male QALE varied more across districts than female QALE, and this variation decreased more in males, from
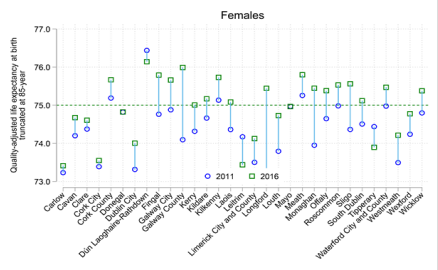
5.2 to 4.3 years between 2011 and 2016. This compares to a decrease from 3.1 years in 2011 to 2.7 in 2016 in females. QALE increased between 2011 and 2016 in the majority of regions within the range from -0.1 to 2.3 years in males, and from -0.7 to 2.2 years in females. However, one district (Westmeath) saw a small reduction in male QALE (-0.1 year) and four districts (Leitrim, Tipperary, Dun Laoghaire-Rathdown
and Mayo) saw reductions in female QALE. Of those districts with decreasing LE or QALE, Dun Laoghaire-Rathdown was the only district above the 2016-QALE average.
Figure 3 : Geographic variation and changes over time in quality-adjusted life expectancy at birth until 85 years of age across 31 districts in Ireland, males.
Figure 4 : Geographic variation and changes over time in quality-adjusted life expectancy at birth until 85 years of age across 31 districts in Ireland, females.
Discussion
As a contribution to the debate about health inequalities in Ireland, this study investigated geographic variation in LE and QALE across 31
counties in Ireland by analysing age- and sex-specific population, mortality, and health status data. The average LE until 85 years of age in Ireland in 2016 was high, namely 75.2 years for men and 79.8 years for women. Across the population, 90% reported to be in very good or good health, with lower proportions in the older ages. From 2011 to 2016 LE increased, and so did the proportion of 50- to 84-year-olds in very good or good health.
While the proportion who self-reported very good or good health decreased slightly for both men (-0.3%) and women (-0.1%), a positive trend in self-reported health status was seen between 2011 and 2016 both for men and women aged 50 years and over. In each age group studied within the 50+ population, the proportions of men and women reporting very good or good health increased. Notably, highest increases were seen in the age group with the lowest initial self-reported health status (ages 80 to 84: +3.6% in men and +4.1% in women). Despite these improvements, a quarter of men and women aged 50 years or over reported fair, bad or very bad health status in 2016.
As LE increased and health status remained relatively unchanged overall, QALE improved for men (from 71.6 to 73.6) and women (from 73.9 to 75.0) between 2011 and 2016. However, improvements in LE and QALE occurred at different rates for men and women. Due to larger increases in male than female LE, sex gaps decreased from 3.4 years in 2006 to 2.5 years in 2016 for LE, and from 1.8 years in 2011 to 1.5 in 2016 for QALE, indicating a reduction in health inequalities related to sex.
Substantial geographic variation in LE and self-reported health was observed across counties. The geographic variation in LE was larger in men than women, but this difference decreased over time. In 2011, also QALE differed across geographic districts. While QALE had increased in most districts by 2016, the rate of increase differed and geographic variation remained, highlighting the regional health inequalities that
exist across Ireland, and the need to identify their underlying causes.
According to Irish projections, population growth and an increase in LE will accelerate healthcare costs in Ireland in the coming decade. In particular, the share of the youngest and eldest population groups is expected to increase [21]. Both of these groups are eligible for free healthcare provision and medication in Ireland, either through medical cards or the General Practitioner Visit Cards scheme, thereby posing costs on the healthcare system. The projections furthermore revealed regional differences in costs occurring through these schemes, with highest use reported and projected for the Midlands region, and lowest in the North-West. The authors identify two possible explanations of this trend, first variation in prevalence of chronic conditions across regions in Ireland, and second higher prescribing of diabetes medication previously observed in the Midlands [21,32,33]. It is notable that the Midlands also were identified as an area with relatively low availability of health services, such as physiotherapists [34], and that rates of surgical procedures vary considerably across counties in Ireland [35-37].
Also, in the United States, differences in healthcare use were seen that, together with health behaviour and differences in health-related government expenditures, explained geographic variation in health [9,38]. Other studies found regional differences in mortality related to chronic diseases, self-harm, injuries and drug use as well as differences in population well-being [8,39-41]. Other potential reasons for geographic variation within countries are socioeconomic differences, such as seen in the United States, Taiwan and Germany, race (US and Taiwan), poverty, deprivation and food insecurity (US) and urbanisation (Portugal) [7,9,38,42-45]. Rural regions tend to see lower LE than cities, likely due to lower access to healthcare and health-promoting factors [43]. For example, a review of injury-related health outcomes showed that mortality was higher in rural than urban regions, which was solely explained by a higher rural pre-hospital mortality, whereas the in-hospital mortality was similar between urban and rural patients [46]. Also in Ireland, rural-urban differences in emergency admissions were observed among older adults. These were more common in relatively rural counties compared to larger cities. Additionally, residents in rural areas in Ireland may have insufficient access to primary healthcare [47]. Differences in smoking, physical activity levels and obesity prevalence further explained geographic differences in life expectancy between US counties [7]. Additionally, in the US, a study found that the same 22 socio-economic and environmental variables explained geographic differences in premature mortality as racial differences, indicating that various inequalities might be reduced, if these factors were targeted cumulatively [42].
Regional differences in LE and health have been identified in previous Irish studies. Abdalla et al. compared the Survey of Lifestyle, Attitude and Nutrition 2007 data (n=10364), as well as the 2006 Census and 2007 mortality data used in this study, to reported health and mortality in a census study of the Irish Traveller community (n=5288) [48]. The study concluded that Irish Travellers have a shorter LE, healthy LE and disability-free LE than the general population, as well as poorer overall health. Chronic conditions, and back pain and arthritis in particular, contributed to these differences. Furthermore, poor health affected the gap between Travellers and the general population in Ireland in women most, whereas premature mortality was the main driver of gaps between men in this study [48]. Accordingly, future studies should investigate disease-specific mortality and LE for geographic differences, which were previously identified from
international cancer registries and studies of cardiovascular diseases among others [45,49].
Morrissey et al. matched population survey, census data and hospital record data with small area population statistics and identified differences in acute hospitalisation across Irish regions and electoral districts [20]. In particular, they found highest levels in the Northwest, West and Mid-west of Ireland, and they found that districts with high utilisation tend to cluster within a region. While long-term illness, age and, to a lesser degree, education explained some of the variation in hospitalisation in this study, a large proportion of variation remained unexplained [20]. Notably, this contrasts with recent findings that coverage of hospital emergency care resources is highest in the Northeast of Ireland, with wide disparities between counties in per-capita investments for these services [50]. Accordingly, geographic differences in healthcare demand need to be assessed beyond mere consideration of population density, long-term illness and age when allocating health resources and aiming to increase health equity in Ireland [20,50].
Nevertheless, population density, chronic conditions and age remain important parameters when assessing healthcare need, and mapping these parameters within small areas can help direct future investment to those places where they are needed most. For example, a recent study mapped these parameters in relation to dementia care and thereby identified geographic areas where demand is high and access to dementia services relatively low in comparison to other areas in the country [51]. In fact, more emphasis on regional and local health development is promoted through the National Healthy Cities and Counties of Ireland Network, which was implemented in the 31 Irish city or county councils since its launch in 2016. The initiative seeks to improve quality of life and well-being, with local projects to inform national policymaking [52]. This presents an excellent opportunity for future studies to identify and tackle individual contributors to health inequalities and thereby reduce the geographic variation in LE and QALE seen in this study.
Strengths
A major strength of this study is the comprehensive, national nature of the data. Furthermore, the availability of data from multiple time points and pragmatic linkage techniques allowed us to analyse trends over time.
Limitations
Age- and sex-specific population data on county level were only available during the census years (i.e. 2006, 2011 and 2016). More detailed data would have allowed us to use more sophisticated analytic approaches, although the ideal level of aggregation is unclear. In the US, where county size tends to exceed that of Irish counties, use of sub-county level data was recommended to study geographic differences in LE using census data and most geographic variation there was found on local level [53,54]. However, small-area
population statistics are more sensitive to population shifts, for example when comparing areas with high or low density of nursing homes [55].
Conclusion
Substantial differences in self-reported health status, LE and QALE exist in Ireland across sexes, age groups and 31 counties. From 2006 to 2016, LE, the health status of 50- to 84-year-olds, and QALE improved. While sex differences in geographic variation decreased mainly due to health and LE increases in males, decreases in LE and QALE observed among females in four districts require further investigation. Despite overall improvements, geographic variation in LE, in QALE and in sex differences of either remained in 2016 and need to be addressed through future study, regional policies and health promotion.
Data availability
Data available from the authors upon request.
Conflicts of Interest
None to report.
References
Seniori Costantini A, Gallo F, Pega F, Saracci R, Veerus P, West R. Population health and status of epidemiology in Western European, Balkan and Baltic countries. Int J Epidemiol. 2015;44(1):300-23.
Newton JN, Briggs AD, Murray CJ, Dicker D, Foreman KJ, Wang H, et al. Changes in health in England, with analysis by English regions and areas of deprivation, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;386(10010):2257-74.
Gondos A, Bray F, Brewster DH, Coebergh JW, Hakulinen T, Janssen-Heijnen ML, et al. Recent trends in cancer survival across Europe between 2000 and 2004: a model-based period analysis from 12 cancer registries. Eur J Cancer. 2008;44(10):1463-75.
Szwarcwald CL, Souza Júnior PR, Marques AP, Almeida WD, Montilla DE. Inequalities in healthy life expectancy by Brazilian geographic regions: findings from the National Health Survey, 2013. Int J Equity Health. 2016;15:1-9.
Kim S, Yi S, Kim M, Kim B, Lee H, Jeon T, Cho Y. Unequal geographic distribution of life expectancy in Seoul. Asia Pac J Public Health. 2015;27(2):NP1002-12.
Eslava-Schmalbach JH, Rincón CJ, Guarnizo-Herrero CC. Life expectancy at birth in Colombia, 2000-2009: inequalities by region and gender. Biomedica. 2013;33(3):383-92.
Xie Y, Bowe B, Yan Y, Cai M, Al-Aly Z. County-level contextual characteristics and disparities in life expectancy. Mayo Clin Proc. 2021;96(1):92-104.
Singh GK, Kogan MD, Slifkin RT. Widening disparities in infant mortality and life expectancy between Appalachia and the rest of the United States, 1990–2013. Health Aff. 2017;36(8):1423-32.
Dwyer-Lindgren L, Bertozzi-Villa A, Stubbs RW, Morozoff C, Mackenbach JP, van Lenthe FJ, et al. Inequalities in life expectancy among US counties, 1980 to 2014: temporal trends and key drivers. JAMA Intern Med. 2017;177(7):1003-11.
Skaftun EK, Verguet S, Norheim OF, Johansson KA. Geographic health inequalities in Norway: a Gini analysis of cross-county differences in mortality from 1980 to 2014. Int J Equity Health. 2018;17(1):1-8.
Kalkınma E, Örgütü İ. Health at a Glance 2019 OECD Indicators.
McCarthy A, Kirke P. Absolute and socioeconomically stratified trends in birth rate and infant mortality rate in Ireland 1984–2005. Ir J Med Sci. 2010;179:561-8.
Dockery DW, Rich DQ, Goodman PG, Clancy L, Ohman-Strickland P, George P, et al. Effect of air pollution control on mortality and hospital admissions in Ireland. Res Rep Health Eff Inst. 2013;(176):3-109.
Murphy SM, Kieran I, Shaughnessy MO. The trauma of a recession. Ir J Med Sci. 2011;180:735-6.
Masterson S, Wright P, O’donnell C, Vellinga A, Murphy AW, Hennelly D, et al. Urban and rural differences in out-of-hospital cardiac arrest in Ireland. Resuscitation. 2015;91:42-7.
Sharp L, Donnelly D, Hegarty A, Carsin AE, Deady S, McCluskey N, et al. Risk of several cancers is higher in urban areas after adjusting for socioeconomic status. Results from a two-country population-based study of 18 common cancers. J Urban Health. 2014;91:510-25.
O’farrell IB, Corcoran P, Perry IJ. The area level association between suicide, deprivation, social fragmentation and population density in the Republic of Ireland: a national study. Soc Psychiatry Psychiatr Epidemiol. 2016;51:839-47.
Corcoran P, Arensman E. Suicide and employment status during Ireland’s Celtic Tiger economy. Eur J Public Health. 2011;21(2):209-14.
Morrissey K, O’Donoghue C, Clarke G, Li J. Using simulated data to examine the determinants of acute hospital demand at the small area level. Geographical Analysis. 2013;45(1):49-76.
Morrissey K, O’Donoghue C, Clarke G, Li J. Using simulated data to examine the determinants of acute hospital demand at the small area level. Geographical Analysis. 2013;45(1):49-76.
Conway A, Kenneally M, Woods N, Thummel A, Ryan M. The implications of regional and national demographic projections for future GMS costs in Ireland through to 2026. BMC Health Serv Res. 2014;14(1):1-0.
Layte R, Banks J. Socioeconomic differentials in mortality by cause of death in the Republic of Ireland, 1984–2008. Eur J Public Health. 2016;26(3):451-8.
Walsh PM, Byrne J, Kelly M, McDevitt J, Comber H. Socioeconomic disparity in survival after breast cancer in Ireland: observational study. PLoS One. 2014;9(11):e111729.
Smyth B, Evans DS, Kelly A, Cullen L, O’donovan D. The farming population in Ireland: mortality trends during the ‘Celtic Tiger’ years. Eur J Public Health. 2013;23(1):50-5.
McGee HM, Hevey D, Horgan JH. Cardiac rehabilitation service provision in Ireland: the Irish Association of Cardiac Rehabilitation survey. Ir J Med Sci. 2001;170:159-62.
Lavin D, Hevey D, McGee HM, De La Harpe D, Kiernan M, Shelley E. Cardiac rehabilitation services in Ireland: the impact of a coordinated national development strategy. Ir J Med Sci. 2005;174:33-8.
Central Statistics Office, Mortality differentials in Ireland. 2010.
Central Statistics Office, Standard documentation metainformation on population and migration estimates. 2018, Central Statistics Office: Cork, Ireland.
Szende A, Janssen B, Cabases J. Self-reported population health: an international perspective based on EQ-5D.
Naughton C, Bennett K, Feely J. Prevalence of chronic disease in the elderly based on a national pharmacy claims database. Age Ageing. 2006;35(6):633-6.
Usher C, Bennett K, Feely J. Regional variation in the prescribing for diabetes and use of secondary preventative therapies in Ireland. Pharmacoepidemiol Drug Saf. 2005;14(8):537-44.
Eighan J, Walsh B, Smith S, Wren MA, Barron S, Morgenroth E. A profile of physiotherapy supply in Ireland. Ir J Med Sci. 2019;188:19-27.
Ahmed O, Mealy K, Kelliher G, Keane F, Sorensen J. Exploring geographical variation in access to general surgery in Ireland: evidence from a national study. Surgeon. 2019;17(3):139-45.
Ahmed O, Mealy K, Sorensen J. Exploring geographic variation in acute appendectomy in Ireland: results from a national registry study. BMJ Open. 2019;9(8):e025231.
Walsh ME, Boland F, O’Byrne JM, Fahey T. Geographical variation in musculoskeletal surgical care in public hospitals in Ireland: a repeated cross-sectional study. BMJ Open. 2019;9(5):e028037.
Chetty R, Stepner M, Abraham S, Lin S, Scuderi B, Turner N, Bergeron A, Cutler D. The association between income and life expectancy in the United States, 2001-2014. JAMA. 2016;315(16):1750-66.
Voeks JH, McClure LA, Go RC, Prineas RJ, Cushman M, Kissela BM, et al. Regional differences in diabetes as a possible contributor to the geographic disparity in stroke mortality: the REasons for Geographic And Racial Differences in Stroke Study. Stroke. 2008;39(6):1675-80.
Glynn PA, Molsberry R, Harrington K, Shah NS, Petito LC, Yancy CW, et al. Geographic variation in trends and disparities in heart failure mortality in the United States, 1999 to 2017. J Am Heart Assoc. 2021;10(9):e020541.
Arora A, Spatz E, Herrin J, Riley C, Roy B, Kell K, Coberley C, Rula E, Krumholz HM. Population well-being measures help explain geographic disparities in life expectancy at the county level. Health Aff (Millwood). 2016;35(11):2075-82.
Cullen MR, Cummins C, Fuchs VR. Geographic and racial variation in premature mortality in the US: analyzing the disparities. PLoS One. 2012;7(4):e32930.
Weng SS, Chan TC, Hsu PY, Niu SF. Neighbourhood Social Determinants of health and geographical inequalities in premature mortality in Taiwan: A spatiotemporal approach. Int J Environ Res Public Health. 2021;18(13):7091.
Kuhn J. Gesundheitswesen. 2006. 68(8-9):551-6.
Araújo C, Pereira M, Viana M, Rocha OL, Bennett K, Lunet N, et al. Regional variation in coronary heart disease mortality trends in Portugal, 1981-2012. Int J Cardiol. 2016;224:279-85.
Keeves J, Ekegren CL, Beck B, Gabbe BJ. The relationship between geographic location and outcomes following injury: A scoping review. Injury. 2019;50(11):1826-38.
Walsh ME, Cronin S, Boland F, Ebell MH, Fahey T, Wallace E. Geographical variation of emergency hospital admissions for ambulatory care sensitive conditions in older adults in Ireland 2012–2016. BMJ Open. 2021;11(5):e042779.
Abdalla S, Kelleher CC, Quirke B, Daly L, All-Ireland traveller Health Study team. Disparities in fatal and non-fatal injuries between Irish travellers and the Irish general population are similar to those of other indigenous minorities: a cross-sectional population-based comparative study. BMJ Open. 2013;3(1):e002296.
Baili P, Micheli A, De Angelis R, Weir HK, Francisci S, Santaquilani M, et al. Life tables for world-wide comparison of relative survival for cancer (CONCORD study). Tumori. 2008;94(5):658-68.
Thomas S, Foley C, Kane B, Johnston BM, Lynch B, Smith S, et al. Variation in resource allocation in urgent and emergency Care Systems in Ireland. BMC Health Serv Res. 2019;19:1-1.
Pierse T, Keogh F, Ohea E, Cullinan J. Geographic availability and accessibility of day care services for people with dementia in Ireland. MC Health Serv Res. 2020;20(1):1-9.
Talbot TO, Done DH, Babcock GD. Calculating census tract-based life expectancy in New York state: a generalizable approach. Popul Health Metr. 2018;16:1-3.
Boing AF, Boing AC, Cordes J, Kim R, Subramanian SV. Quantifying and explaining variation in life expectancy at census tract, county, and state levels in the United States. Proc Natl Acad Sci U S A. 2020;117(30):17688-94.
Veugelers PJ, Hornibrook S. Small area comparisons of health: applications for policy makers and challenges for researchers. Chronic Dis Can. 2002;23(3):100.
Supplementary Material
2006 N(%)*
2011 N(%)*
2016 N(%)*
Total
4239848 (100%)
4588252 (100%)
4761865 (100%)
Sex
Men
2121171 (50.0%)
2272699 (49.5%)
2354428(49.4%)
Women
2118677 (50.0%)
2315553 (50.5%)
2407437 (50.6%)
Age
0-4 years
302252 (7.1%)
356329 (7.8%)
331515 (7.0%)
5-9 years
288325 (6.8%)
320770 (7.0%)
355561 (7.5%)
10-14 years
273872 (6.5%)
302491 (6.6%)
319476 (6.7%)
15-19 years
290257 (6.8%)
283019 (6.2%)
302816 (6.4%)
20-24 years
342475 (8.1%)
297231 (6.5%)
273636 (5.7%)
25-29 years
373078 (8.8%)
361122 (7.9%)
297435 (6.2%)
30-34 years
349361 (8.2%)
393945 (8.6%)
361975 (7.6%)
35-39 years
322105 (7.6%)
364261 (7.9%)
389421 (8.2%)
40-44 years
301329 (7.1%)
330812 (7.2%)
357460 (7.5%)
45-49 years
274745 (6.5%)
305185 (6.7%)
326110 (6.8%)
50-54 years
247068 (5.8%)
274386 (6.0%)
299935 (6.3%)
55-59 years
225328 (5.3%)
244522 (5.3%)
270102 (5.7%)
60-64 years
181727 (4.3%)
218786 (4.8%)
238856 (5.0%)
65-69 years
143396 (3.4%)
173638 (3.8%)
211236 (4.4%)
70-74 years
119152 (2.8%)
131190 (2.9%)
162272 (3.4%)
75-79 years
92466 (2.2%)
102036 (2.2%)
115467 (2.4%)
80-84 years
64884 (1.5%)
70113 (1.5%)
81037 (1.7%)
≥ 85 years
48028 (1.1%)
58416 (1.3%)
67555 (1.4%)
Urban/rural region
Urban
2574313 (60.7%)
2846882 (62.0%)
2985781 (62.7%)
Rural
1665535 (39.3%)
1741370 (38.0%)
1776084 (37.3%)
Self-reported health
Very good
N/A
2767681 (60.3%)
2827544 (58.1%)
Good
N/A
1282956 (28.0%)
1316467 (26.9%)
Fair
N/A
368131 (8.0%)
382905 (7.7%)
Bad
N/A
57243 (1.2%)
62697 (1.2%)
Very bad
N/A
12418 (0.3%)
13738 (0.3%)
Missing
N/A
99823 (2.2%)
158514 (2.1%)
Deaths
28117**
28274
28380
Mortality rate by 1,000
6.6
6.2
6
* % of total responses for this variable and ** 2007 data as 2006 was not available. Appendix 1 : Population characteristics from Census of Population and death registries in 2006-2016.
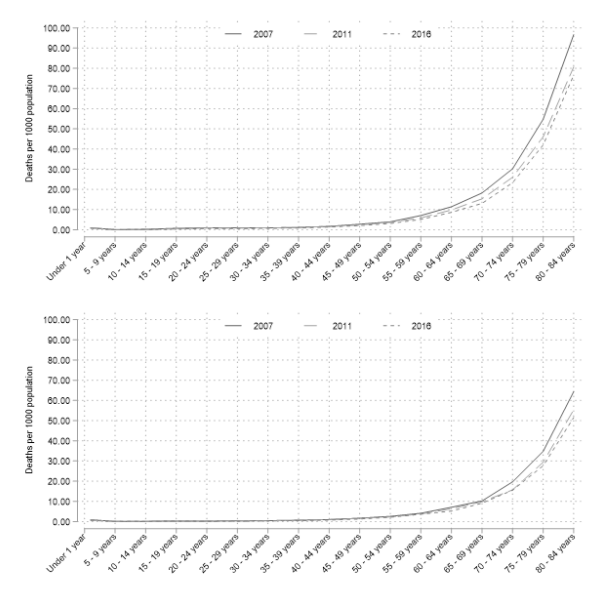
Appendix 2 : Changes in mortality in Ireland from 2007 to 2016.
Age
% very good or good health in 2011
% very good or good health in 2016
Change in % points
Change in % points
Male
Female
Male
Female
Male
p-value
Female
p-value
0-4 years
98.6%
98.9%
98.5%
98.9%
-0.1%
0.78
0.0%
0.459
5-9 years
98.6%
98.9%
98.4%
98.9%
-0.2%
0.275
0.0%
<0.001
10-14 years
98.7%
99.0%
98.6%
98.7%
-0.1%
<0.001
-0.3%
0.001
15-19 years
98.2%
97.8%
97.7%
97.2%
-0.5%
<0.001
-0.6%
<0.001
20-24 years
96.8%
96.5%
96.5%
96.0%
-0.3%
<0.001
-0.5%
<0.001
25-29 years
95.9%
95.8%
95.7%
95.5%
-0.2%
<0.001
-0.3%
0.008
30-34 years
95.0%
95.1%
94.8%
94.8%
-0.2%
<0.001
-0.3%
0.004
35-39 years
93.7%
93.7%
93.8%
93.5%
0.1%
0.016
-0.2%
0.165
40-44 years
92.2%
92.2%
92.2%
91.9%
0.0%
0.002
-0.3%
0.585
45-49 years
90.1%
90.1%
90.1%
90.1%
0.0%
0.851
0.0%
0.925
50-54 years
86.9%
87.0%
87.5%
87.6%
0.6%
<0.001
0.6%
<0.001
55-59 years
81.7%
82.8%
83.5%
84.4%
1.8%
<0.001
1.6%
<0.001
60-64 years
76.5%
79.5%
78.3%
80.9%
1.8%
<0.001
1.4%
<0.001
65-59 years
75.1%
77.0%
76.2%
79.0%
1.1%
<0.001
2.0%
<0.001
70-74 years
71.7%
71.9%
73.6%
74.6%
1.9%
<0.001
2.7%
<0.001
75-79 years
64.9%
63.4%
68.1%
67.0%
3.2%
<0.001
3.6%
<0.001
80-84 years
57.2%
53.7%
60.8%
57.8%
3.6%
<0.001
4.1%
<0.001
85 years +
48.3%
43.0%
51.1%
45.1%
2.8%
<0.001
2.1%
<0.001
Total
90.6%
89.9%
90.3%
89.8%
-0.3%
<0.001
-0.1%
<0.001
* % of total responses for this variable and ** 2007 data as 2006 was not available. Appendix 3: Proportion of the Irish population in very good or good health by year, sex and age group. Changes in percentage points and p-values are shown to indicate significance of change.
Appendix 4 : Changes in the proportion of very good or good self-reported health state in Ireland from 2011 to 2016.